
Subacute sclerosing panencephalitis

A prominent member of the North American homeopathic community recently posted a link to this article:
Measles Took My Daughter. This Is What I Want Everyone to Know.
This described a case of subacute sclerosing panencephalitis (SSPE), an invariably fatal disease, in a 10-year old girl in 2023, occurring following acute measles infection at age 5 months in 2013 in Manchester, England.
With the comment:
“Well, it seems that America’s pre-RFK vaccine policies and modern medical treatment killed this child … IF this child’s mother had gotten the real measles itself, rather than a vaccine, this mother would have been able to convey measles antibodies to her infant. But once a young girl is vaccinated, she doesn’t create enough measles antibodies to her young infants.
The real BEAUTY of getting the measles is that the mother will be able to protect her infants…”
I’d normally just shrug and give this a pass, but am concerned that it reflects poorly on our profession and might be taken as serious commentary by homeopaths seeking to find grounds for the superiority of our practice.
Let’s look into it:
How does the author know that the mother had been vaccinated, and had not been naturally infected earlier in life, or was merely non-immune? There’s no reference to this in the article, nor to where the mother lived prior to giving birth, nor to her age. It’s probable, based on the mother’s likely age (giving birth to a first child in 2012/2013), that she was born after 1963, likely in the 1980s (we don’t know from the article), so she perhaps received the Hilleman vaccine as a child (tho if her childhood was in the U.K., the vaccination rate in the UK was < 60% in the era a mom giving birth in 2012/2013 was likely a child; there were 139,487 reported notifications of measles in England and Wales in 1980 and 26,180 in 1989). In the U.S., an MMR booster has been recommended to women in their late ’teens in anticipation of pregnancy since the congenital rubella resurgence in 1979, but this is not policy in the U.K.
If the mother had “gotten the real measles itself,” how would we be guaranteed that she, or any of her peers or individuals she infected, would not have been the tragic case(s) of subacute sclerosing panencephalitis sometime over the following 27 years? (the latency of expression ranges months - 27 years, averaging 10 years after acute measles infection); or suffered other serious consequences of measles? It’s quite possible that the child in question might have never been born, or that the mother’s life may have been upended by blindness or hearing loss.
We don’t know the birth & perinatal history of this case - was the child pre-term? (In which case, transplacental passive immunity, which is conferred principally in the late 3rd trimester, would be impaired, & breastfeeding likely problematic). Was she breast or bottle fed? With mom’s or with donated milk? Were there difficulties interfering with breastfeeding, particularly with colostrum at the initiation of breastfeeding, that might have interfered with the transfer of passive immunity?
Did the child (or the mother) have hereditary selective IgA deficiency? (Seen in 0.1-0.2% of children of European heritage; that’d be ~9.6 million cases in the UK in 2013; I’ve seen several cases in my practice).
In any case, passive immunity is (as are all things) imperfect. Even when birthing mothers had near-universal natural childhood exposure to measles, some had inadequate circulating IgG & IgA levels at childbearing age. Memory cells persist, providing maternal protection and some protection of the infant through microchimerisms, but maternal circulating antibodies, the principal agents of passive immunity, wane slowly over time (at 0.04% per year) following both naturally-acquired and vaccine-acquired immunity. The transmission of passive immunity to infants appeared to have been somewhat more effective in the pre-vaccine era (but still not 100%), likely due to periodic “boosting” of maternal IgG and IgA levels from asymptomatic exposure to measles circulating in the community, an effect that can be emulated at lower risk to the community at large with an MMR in adolescence or prior to a planned pregnancy (as an attenuated “live” virus vaccine, the MMR is not given in pregnancy out of an abundance of caution, although inadvertent administration in unidentified early pregnancies has not resulted in adverse consequences).
Neonatal measles (in the 1st 28 days following birth) is extremely rare, and infants under 6 months often have some protection from maternal antibodies, but this wanes over the first 6 months, leaving infants aged 6–12 months highly vulnerable; 70% of infants born with passive immunity at birth become seronegative and susceptible to measles by 4 months, with 90% to 100% susceptible by 6 months, whether maternal immunity was acquired naturally or via vaccination. In regions with poor vaccination coverage, 4.3% of measles cases occur in children under 6 months of age and Infants younger than 12 months are frequently involved in outbreaks, with cases in young infants ranging from 0.25% to 83% of total outbreak cases. Not insignificant percentages. & A high viral load may overwhelm even ordinarily adequate immunity. The child mentioned in the referenced article contracted measles in a large local outbreak (1,000 cases in Manchester, England) at 7 months.
The author of the comment went on to suggest:
Instead, to make things worse, the doctor recommended that the child take Tylenol, a drug that is known (!) to suppress fever...and fever is an important, even vital, defense of the body in its efforts to fight infection … In other words, this SUPPRESSION of fever led to this child’s inability to fight the measles infection.”
There is NO evidence that “suppression” of fever contributes to the development of subacute sclerosing panencephalitis, in this case or in any other. The disease, described in 1933 (likely previously regarded as a mysterious illness) and definitively linked to measles virus in 1969 (the measles virus was first cultured, isolated, & identified in 1954) results from mutated copies of wild type measles virus with restricted expression of the genes encoding for viral envelope proteins, permitting the defective virus to survive persistently in the CNS without evoking an immune response, taking up latent infection in CNS neurons and glial cells. It has never been observed to involve vaccine-strain virus, and the incidence has plummeted since the adoption of the measles vaccine. The author’s confident assertion that “this SUPPRESSION of fever led to this child’s inability to fight the measles infection” is founded purely in their imagination, parroting “settled homeopathic canon” (dogma) in invoking “suppression” by conventional medications (acetaminophen/paracetamol in this case) as the root of all evil. It’s true that “fever is an important, even vital, defense of the body in its efforts to fight infection,” but the impact is seen with modest pyrexia or even the modest elevation of core temperature from a warm bath, and is not enhanced by excessive fever; we’re not told the extent of fever or how aggressive fever management might have been in this case, but typically the fever of measles is extreme (often over 104°F/40 °C) and the metric of treatment is comfort and reduced distress, with reduction of temperature short of “normalization.”
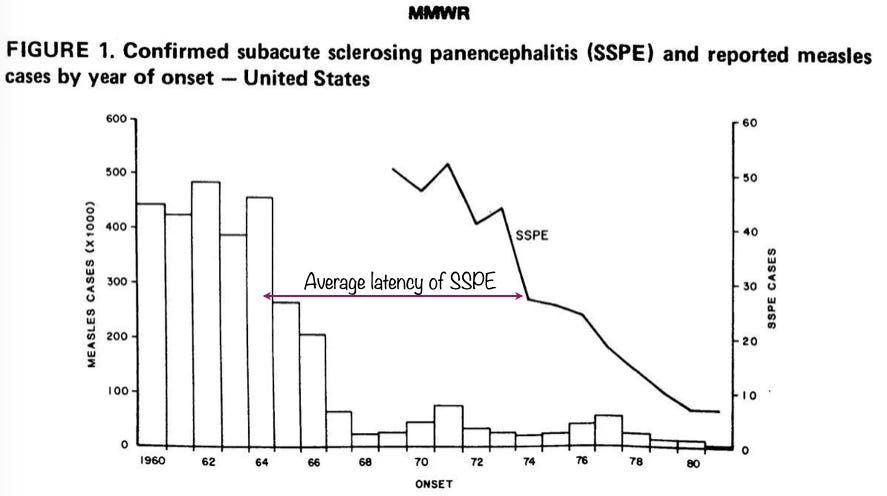
The most important takeaway from this story, is that measles is to be respected as a potentially serious disease with both short- and long-term consequences. This is but one anecdote; despite its near-eradication in the post-vaccine era, we still see 4-5 cases annually of subacute sclerosing panencephalitis in the U.S., most of these as remnants of old cases when measles was more prevalent (the lag time to the first appearance of symptoms averages 10 years, ranging from months to 27 years following acute measles infection). The risk for unvaccinated infants under 15 months is as high as 1 in 609 cases of measles (1 in 5,000 cases in individuals infected later in life). The incidence has declined precipitously since the adoption of measles vaccination, from 50 reported cases in the U.S. in 1970; a national SSPE registry was only initiated in the U.S. in 1969; we don’t have reasonable records prior to 1970:
The most recently reported case in North America, was reported in February, 2016, in a 7-year-old boy who had contracted measles in Afghanistan at 5 months, where MMR coverage is only ~50-60% and measles is endemic.
In the UK, after 15 years with no pediatric UK-acquired cases, between May 1997 and December 2019, 8 pediatric SSPE cases were reported with a history of UK-acquired measles.
For those unfamiliar with the disease, after an asymptomatic period of 1 month to 27 years (avg. 10 years) following acute measles infection (during which time there exist no means of prediction of occurrence), progressive neurological deterioration occurs, beginning with nonspecific neurological symptoms including a range of behavioral changes and intellectual problems, lethargy and speech problems, followed by myoclonic seizures, blindness, ataxia, dementia, and eventually (invariably) death.
Stage 1: Personality changes, mood swings, or depression, often with fever, headache, and memory loss. This begins with subtle changes such as general inattention or struggling with schoolwork, often interpreted as depression or stress, with diagnosis rarely made prior to stage 2.
Stage 2: Typically 6 months after initial symptom onset, jerking, muscle spasms, seizures, loss of vision, visual hallucinations, confusion, and dementia.
Stage 3: Jerking movements are replaced by writhing (twisting) movements and rigidity, possible blindness or death.
Stage 4: Progressive loss of consciousness into a persistent vegetative state, which may be preceded by or concomitant with paralysis, with impaired regulation of breathing, heart rate, and blood pressure. Death usually occurs as a result of fever, heart failure, or autonomic nervous system collapse.
A fictional account is portrayed in episode 2 of season 1 (titled ”Paternity”) of the TV drama House, initially suspected successively to involve traumatic brain injury, multiple sclerosis, and neurosyphilis, eventually treated with intrathecal interferon, a fictional treatment.
The antiviral drug isoprinosine, if started early in stage 1, may stabilize or improve symptoms in ~ 30% of cases, but its impact is rarely impressive. Interferon alfa, amantadine, ribavirin, and immunoglobulin therapy have been used with extremely limited benefit. Anticonvulsants may be used in symptomatic management. Following the onset of stage 2, when it is most commonly identified, the disease is invariably fatal.
The U.S. hospitalization rate of acute measles is 5-20%, with a financial cost of $4,000 - $46,000 per patient, with pneumonia in 5%, acute encephalitis in 0.1%, sensorineural hearing loss in 10%, and acute demyelinating encephalomyelitis in 0.1% of cases (acute measles encephalitis, acute demyelinating encephalomyelitis, and subacute sclerosing panencephalitis are distinct maladies all related to measles), with a mortality rate of 0.1%–0.3%. The risk of subacute sclerosing panencephalitis ranges from 0.16% in infants infected with measles under 15 months to 0.0002% in individuals infected later in life. Those %ages may seem small compared to the mortality rate of gun violence, but for a highly communicable disease with the potential to infect an entire birth cohort, the numbers become enormous. In the immediate pre-vaccine era of the 1950s, following the dramatic reduction in all-cause childhood mortality from the 1800s through the 1940s, these added up to over 500,000 annual measles cases with ~50,000 annual acute hospitalizations and ~ 500 annual childhood deaths, not counting the estimated 50+ annual cases of subacute sclerosing panencephalitis spread over the subsequent 27 years and the contribution of measles-induced immune amnesia to non-measles morbidity & mortality.
It would seem callous to reduce the societal cost of measles to mere financial figures, but these are realities in the society we deal with. It’s estimated that the U.S. measles outbreaks of 2025 alone cost more than $244 million, with a projected annual financial cost of measles of $1.5 billion by 2030.

I’d like to put out a plea that homeopaths who wish to emphasize the great value of our profession do so by cultivating their personal proficiency in practice rather than by focusing on the denigration of other approaches to healthcare, particularly on topics they understand poorly. Our own profession suffers from misrepresentation by individuals unfamiliar with its intricacies, willing to speak beyond the extent of their knowledge. Analyses such as that of the author of the referenced commentary merely expose us to ridicule, in this case deservedly so. The success of homeopathy is a function of the individual practitioner, and our value is best demonstrated in the fruits of our practice rather than in dogmatic claims of the inadequacies of other approaches.